Facial Anatomy for Safe Injecting: The Danger Zones
The face is a densely vascular structure, and its arteries connect, through the angular and dorsal nasal vessels, with the ophthalmic circulation. That connection is why filler placed carelessly in the wrong region can, in rare cases, travel to the eye and cause blindness. It is also why we teach the facial danger zones as a defined framework — regions where the vessels at risk, and the consequences of occluding them, demand particular respect.
This guide walks through the facial danger zones we teach at PHP Training Academy, the vessels at risk in each, and the principles that keep injecting safe.
Why anatomy sits at the centre of safe practice
Injecting is a blind procedure. You cannot see the artery beneath the skin — you can only know, from your anatomical understanding, where it is likely to run, how deep it sits, and how its position varies between patients. Good injectors build a three-dimensional mental map of the face and inject around that map, choosing planes and techniques that keep the needle or cannula tip away from the vessels that matter.
This is knowledge you apply on every single patient, not just in emergencies. It informs your injection depth, your choice of needle versus cannula, your entry points, your vectors, and the volume you deposit in any one place. It also underpins the UK safety standards set out by bodies such as the Joint Council for Cosmetic Practitioners, which place anatomical competence at the core of safe practice.
The key facial danger zones
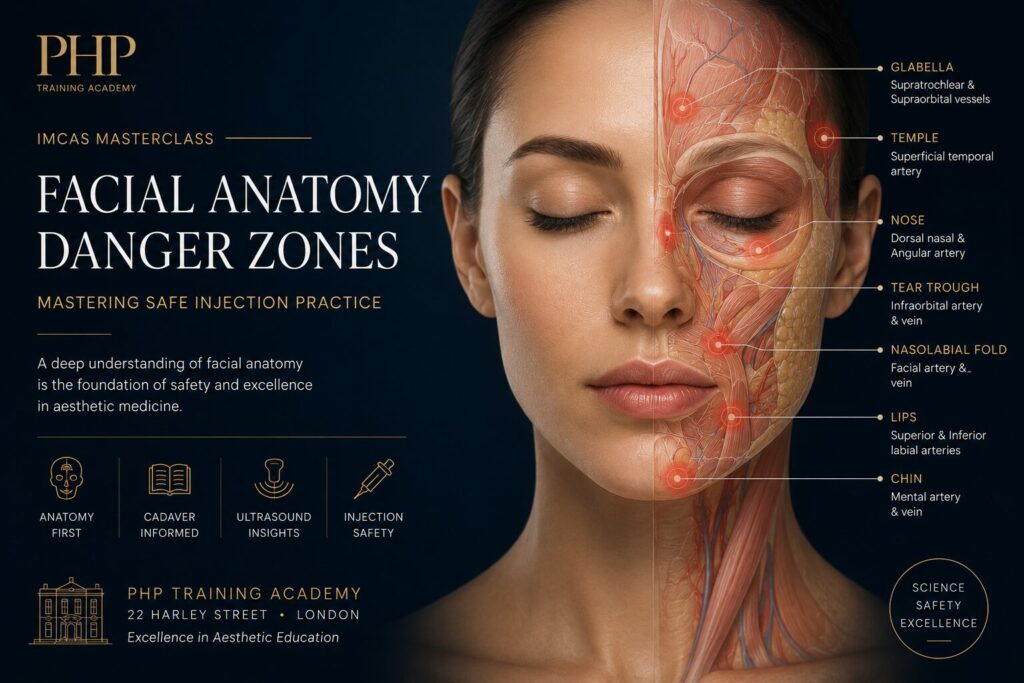
1. The glabella
The glabellar region — between the brows — is the highest-risk area on the face for visual complications. The supratrochlear and supraorbital arteries run here, in direct communication with the ophthalmic artery. Filler forced into these vessels has a route straight to the retinal circulation. Superficial injection, low volumes, low pressure and extreme caution are essential, and many practitioners avoid filler here altogether in favour of alternatives.
2. The nose
The nasal dorsum and tip are supplied by the dorsal nasal and lateral nasal arteries, again connected to the ophthalmic system. The nose has poor collateral circulation, which means an occlusion here can rapidly progress to skin necrosis of the tip, as well as carrying blindness risk. Non-surgical rhinoplasty is an advanced procedure for good reason — the margin for error is small.
3. The nasolabial fold and nasal ala
The angular artery, a continuation of the facial artery, ascends alongside the nose towards the medial canthus. Its course is variable and its depth changes as it rises, making the nasolabial fold and the base of the ala a classic site for inadvertent intravascular injection. Blanching along the side of the nose after fold treatment is a warning sign that must never be ignored.
4. The forehead and temple
The forehead carries the supratrochlear and supraorbital arteries as they emerge and travel upward, while the temple region overlies the superficial temporal artery and a network of vessels running across several tissue planes. The temple is anatomically complex, with vessels at different depths, and demands careful plane selection and technique.
5. The infraorbital region and tear trough
The under-eye and tear trough area sits close to the infraorbital artery as it exits the infraorbital foramen, and to the angular artery medially. The skin here is thin and unforgiving, complications are highly visible, and the proximity to the orbit raises the stakes. This is widely regarded as an advanced area that should not be attempted early in a practitioner’s development.
A note on the lips
While often taught separately from the classical facial danger zones, the lips deserve a mention: the superior and inferior labial arteries run within the lip body and are a common site of vascular events during lip augmentation. High treatment volumes across the sector make lip work a frequent source of occlusions, even if the systemic consequences are usually less severe than in the glabella or nose.
Turning anatomy into safe technique
Knowing where the vessels are is only useful if it changes what your hands do. The principles that translate anatomical knowledge into safety include:
Inject in the correct plane. Knowing whether a vessel runs superficially or deep in a given area lets you choose a plane that avoids it.
Consider a cannula in higher-risk zones. A blunt-tipped cannula is more likely to push a vessel aside than to enter it, though it does not remove risk entirely.
Use low volumes and low pressure. Small aliquots, deposited slowly, limit the amount of product that can enter a vessel and the force behind it.
Keep the tip moving. Depositing product while withdrawing, rather than delivering a large static bolus, reduces the chance of filling a vessel.
Aspirate where appropriate, and always watch for the immediate signs of compromise — blanching, disproportionate pain, dusky discolouration.
Respect the learning curve. The tear trough, nose, glabella and temple are not areas to attempt before you have mastered lower-risk work under supervision.
Alongside all of this, your consultation and consent process must make the risks of these areas explicit to the patient, and every treatment should end with written aftercare and an emergency contact route. Practitioners should also be fully prepared to manage a vascular event if one occurs — the companion emergency protocol is covered in our guide to managing vascular occlusion.
Where the facial danger zones are truly learned
An article can give you the landmarks and the vocabulary. It cannot give you the dimensional, patient-to-patient feel for facial anatomy that safe injecting requires — that comes from anatomy teaching, cadaveric and imaging study, and supervised hands-on practice on live models. At PHP Training Academy, facial anatomy and the vascular danger zones are taught and assessed as part of our VTCT Skills Level 7 Diploma in Clinical Aesthetic Injectable Treatments, in small groups and under full clinical conditions at our Harley Street training rooms.
The safest injectors are not the ones with the steadiest hands. They are the ones who know, before the needle touches the skin, exactly what lies beneath it.
PHP Training Academy · 22 Harley Street, Suite 8, London W1G 9PL · contact@phptrainingacademy.com · +44 (0)7917 785 695 · www.phptrainingacademy.com
This article is educational guidance for registered healthcare professionals and does not replace accredited hands-on training or your own clinical judgement.


